
Summarizing of our post from last might (which we urge everyone to read) for those who are just now waking up to the global chaos resulting from the B.1.1.529 variant, which today got the Greek letter designation Omicron…
Omicron sounds like the name of an 80s movie's evil Robot King.
— Edward Snowden (@Snowden) November 26, 2021
… skipping the widely expected letter Nu (and certainly the one following it, Xi), here is what we know, courtesy of Newsquawk, Credit Suisse and Citi.
Background
- Regarded as the most heavily mutated variant of the Coronavirus, thus far, as it has 32 mutations in the spike protein and 50 overall. More specifically, scientists have highlighted that there are 10 mutations vs 2 in the Delta variant regarding the receptor binding domain, which is the portion of the virus that makes initial contact with cells.
- The Omicron variant was identified 5 days ago initially in Botswana with subsequent confirmation and sequencing in South Africa with about 100 confirmed cases. Cases have been detected in Israel and Hong Kong and as of this morning, in Belgium.
- Sequencing data suggests 8.1.1.529 has a different evolutionary pathway, but shares a few common mutations with the C.1.2, Beta and Delta variants.
- That said, as we cautioned last night, a significant number of mutations may not necessarily be a ‘negative’ as it is dependent on how these mutations function, which scientists are yet to establish. Then again, since it is the job of science to fearmonger so that Pfizer can buy an even bigger yacht, assume it will be “very very horrifying” until proven innocuous.
Is it more deadly
- It is currently too early to determine if the new variant has higher mortality than previous variants. Reported cases only started rising in South Africa on 19 November, so any impact on hospitalizations and COVID-related deaths will not have yet emerged.
Testing and Detectability
- Tulio de Oliveria, the Director of the Centre for Epidemic Response & innovation (CERI), South Africa, has written that the variant can be detected by a normal PCR test and as such it will be “easy for the world to track it”. It wasn’t immediately clear if this is one of those “excess false positive PCR tests” but it’s safe to assume for now that it is.
- According to Credit Suisse, “one silver lining may come in the ease of identifying this variant via qPCR tests. B.1.1.529 has a deletion within the s-gene which can be identified easily via widely-used PCR tests. More complex sequencing analysis is needed to differentiate the delta variant. This will help track the spread of B.1.1.529, both within Southern Africa and across the globe.”
How widespread is it
- As of Thursday there were almost 100 cases detected in South Africa, where it’s become the dominant strain among new infections. Early PCR test results showed that 90% of 1,100 new cases reported Wednesday in the South African province that includes Johannesburg were caused by the new variant, according to de Oliveira.
- In neighboring Botswana, officials recorded four cases on Monday in people who were fully vaccinated. In Hong Kong, a traveler from South Africa was found to have the variant, and another case was identified in a person quarantined in a hotel room across the hall. Israel has also identified one case in a man who recently traveled to Malawi. Belgium has also reported two new cases.
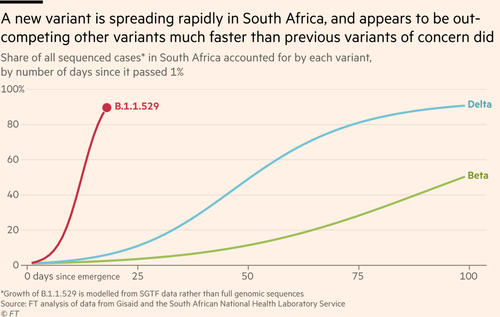
- According to de Oliveira, this new variant, B.1.1.529 “seems to spread very quick! In less than 2 weeks now dominates all infections following a devastating Delta wave in South Africa (Blue new variant, now at 75% of last genomes and soon to reach 100%)”
This new variant, B.1.1.529 seems to spread very quick! In less than 2 weeks now dominates all infections following a devastating Delta wave in South Africa (Blue new variant, now at 75% of last genomes and soon to reach 100%) pic.twitter.com/Z9mde45Qe0
— Tulio de Oliveira (@Tuliodna) November 25, 2021
Transmission
- Oliveria, explains that the new variant is spreading very quickly, in under two-weeks it is now dominating all infections in South Africa following the Delta waves domination – writing that it the variant is “now at 75% of last genomes and soon to reach 100%”.
- Additionally, the virus contains mutations that have been seen in other variants and appear to make transmission easier.
- Outside of Africa, two cases have been reported in Hong Kong, one from a traveller from the region and another who was quarantining in the adjacent hotel room. Most recently, a case has been reported in Israel.
- In response to this, the UK has placed much of southern Africa on the red list, with Israel India, Japan and Singapore also taking similar measures. Additionally, EU Commission President von der Leyen is to propose activation of the emergency air brake, to halt travel from southern Africa.
Vaccines
- It is too early to accurately determine the vaccine response to the new variant. However, the significant number of variants increase the likelihood that current vaccines, which were designed with the original COVID-19 strain in mind, may be less effective.
- Known variants include those that make it more challenging for antibodies to recognise their presence.
- Laboratory testing is already underway according to the South Africa National Institute for Communicable Diseases Initial thoughts from the institute are that partial immune escape is likely, a view that seems possible given the numerous mutations in comparison to the sequence that existing vaccines were designed against. The first view on this to be from in vitro immunogenicity test or perhaps from computer modelling of the sequence. Credit Suisse estimates initial lab data could take less than 1 week to generate given the sequence is already known and work is already ongoing.
New Vaccine Would be Available in 100 days
- According to Pfizer, if a vaccine-escape variant emerges, the company expects to develop, produce a tailor-made vaccine against that variant in 100 days.
Impact of efficacy of existing drugs antibodies is unknown.
- There have been significant advances in treatment of COVID since it emerged in the disease waves of 2020: the use of widely-available steroids, and anti-inflammatory drugs, such as Roche’s Actemra have significantly improved survival outcomes.
- More recently, antibody therapies targeting COVID (LLY, REGN/Roche, AZN) have significantly improved outcomes against COVID variants to date. It will need to be seen if their efficacy is equal against the new B1.1.529 variant.
- Lastly the recent positive data from oral anti-viral agents (PFE, MRK/Ridgeback) may also have the potential to slow the spread of any new waves of COVID. The effectiveness of these treatments against new variants of concern will need to be tested, but lab results should be expected relatively quickly. In-human studies should also yield results relatively quickly if they are run in areas where the prevalence of 8.1.1.529 is high.
What’s next
- According to Citi, concern over Omicron needs to be balanced against the failure of other concerning variants such as Beta (also first identified in Africa) to out-compete delta.
- The next two weeks will be critical to: (i) determine whether Omicron outcompetes delta in high delta prevalence countries (2-3 weeks), (ii) engineered pseudoviruses for Omicron to determine neutralization by serum of vaccination and previously infected patients (2-4 weeks), and (iii) real world data to determine rates of hospitalisation and death (c. 6-8 weeks). The implementation of travel restrictions and public health measures may push back some of the above timeline estimates. Novel oral anti-virals should retain activity against Omicron but resistance may emerge with time.
Via Zerohedge